Foreword - Important
 The information contained in this manual is intended as a fitness guide and is not intended to replace a personal trainer. Remember; please consult your doctor before beginning any type of workout or diet program. Factors unknown to you may have an adverse effect on your physical wellbeing even including death. You may think youre in physical shape to pursue the activities described in this document; only your doctor is qualified to make that decision. Tell him or her that you are planning to begin an exercise program.
The information contained in this manual is intended as a fitness guide and is not intended to replace a personal trainer. Remember; please consult your doctor before beginning any type of workout or diet program. Factors unknown to you may have an adverse effect on your physical wellbeing even including death. You may think youre in physical shape to pursue the activities described in this document; only your doctor is qualified to make that decision. Tell him or her that you are planning to begin an exercise program.
It is important to keep in mind that pain is NOT good especially in joints, bone, chest. Muscles soreness is normal, but not to the point of not being able to use it. NEVER continue a workout with soreness, give the muscles a chance to repair and build. Working out too many times per week can actually make a muscle smaller and weaker if you don't give it a chance to repair. Remember; nutrition is the fuel for work and repair.
In any event, the International Fitness Association (IFA), the author and their representatives cannot assume any responsibility for negative results regardless of how incidental or severe, whether due to an error in this manual or an omission of information. The responsibility is yours. We are not there to see what you're doing; so use common sense. In any event, if you have a question that you can't get answered, send us an email from our website at http://www.ifafitness.com. We'll try to answer your question. A local personal trainer might also be able to help. You don't have to hire a trainer for the long term. You can get a trainer to start you out or just meet you at the gym every couple of weeks to check on your progress and technique (very important). Trainer rates vary from $25/hr to $45/hr and on up. It's a good idea to get your workout program started.
Certification
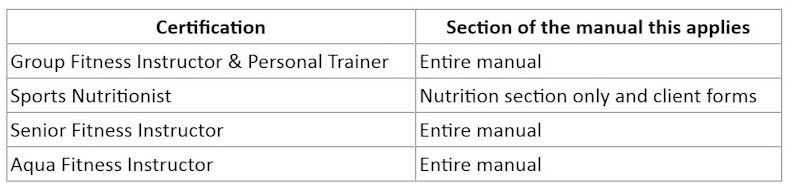
This manual is the course material for the Personal Trainer & Group Fitness Instructor, Health & Fitness Coach, Sports Nutritionist, Senior Fitness Instructor, and Aqua Fitness Instructor certifications. See the table below for specific certification requirements. After reading this manual, you can take the test here on the website and it will be instantly and automatically graded. The results will be sent to IFA automatically. If you pass, you can even pay securely for the certification on the results page of the exam.
|